Introduction
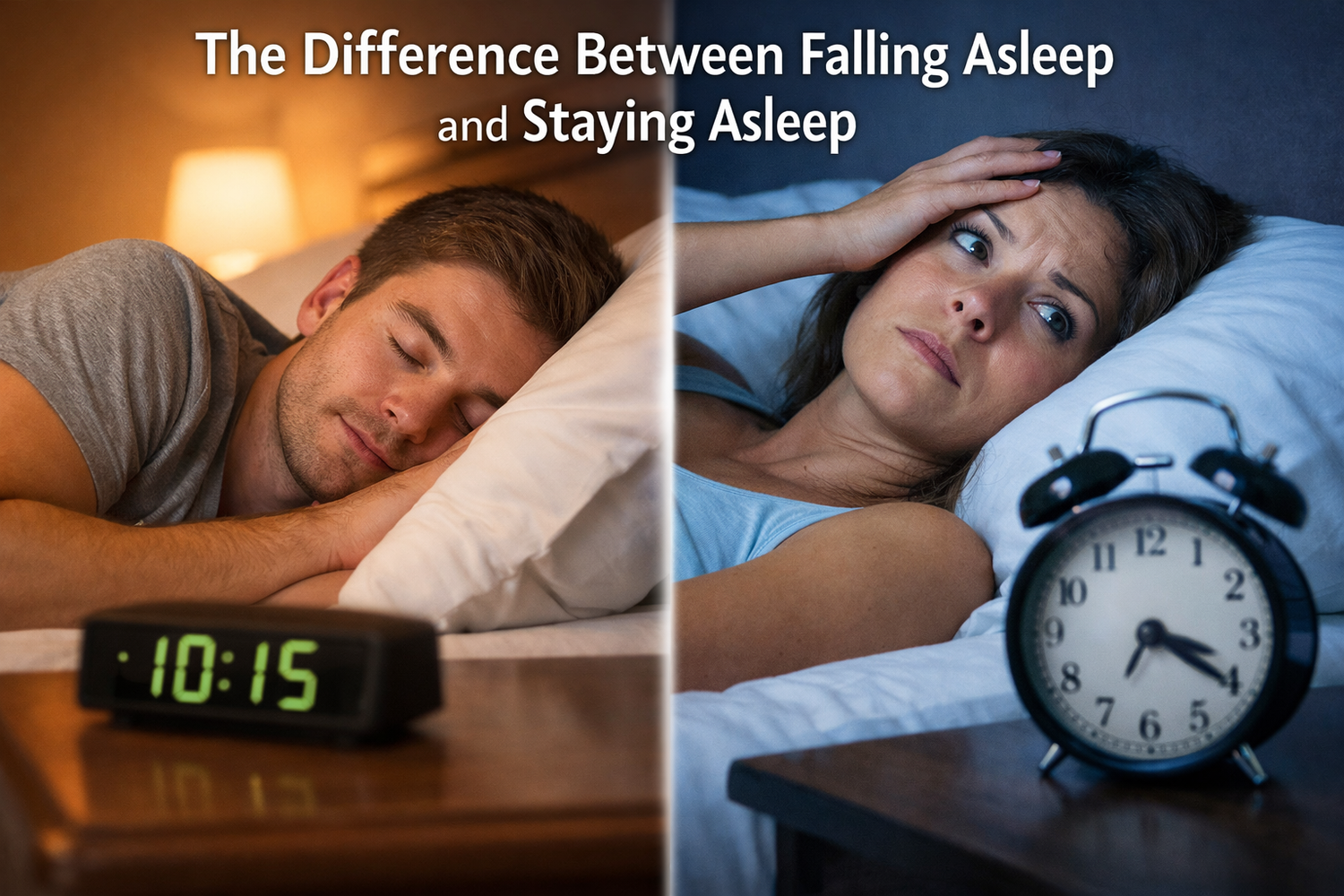
Two people can both say they “sleep badly” and mean completely different things. One lies awake for an hour every night, mind racing, watching the clock. The other drifts off fast, then pops awake at 2 a.m. and stares at the ceiling. On the surface, both have insomnia. Under the hood, falling asleep vs staying asleep are two very different problems.
sleep onset is about how the brain shifts from wake to sleep. Sleep maintenance is about how well that sleep holds through the night. When those get blurred together, people reach for the wrong tools. Someone with early‑night hyperarousal buys a “deep sleep” product meant for middle‑of‑the‑night awakenings. Another person keeps increasing melatonin, hoping it will help them stay asleep, when melatonin is really a timing signal, not an all‑night sedative.
This mix‑up is one reason so many people still feel tired, even after trying pills, teas, apps, and gadgets. If the root issue is misread, the approach rarely works. The good news is that once the difference between falling asleep vs staying asleep is clear, the body becomes much easier to support.
“Sleep is the single most effective thing we can do to reset our brain and body health each day.” — Matthew Walker, PhD, Why We Sleep
This article walks through the science of both phases, the most common causes of each, and how to match strategies to the real problem. Along the way, it explains how SLP1 was built around this exact distinction, with in‑house formulations designed to help people get to sleep smoothly and stay asleep consistently, without sedation or dependency.
Key Takeaways
-
Falling asleep and staying asleep use different brain systems, hormones, and neurotransmitters. Once someone understands which part is breaking down, they can stop guessing, stop stacking random supplements, and focus on the specific levers that actually fit their pattern.
-
Trouble falling asleep usually points to high arousal and mistimed sleep signals, while trouble staying asleep often points to shallow sleep, medical or hormonal triggers, blood sugar swings, or disrupted sleep cycles. These patterns call for different behavioral strategies and different types of nutritional support.
-
SLP1 is built as a three‑part protocol that respects this split. Get to Sleep and the Melatonin Nasal Spray focus on fast, accurate night signaling for sleep onset, while Stay Sleep and Natural Magnesium Sleep Powder support the deeper nervous system state and chemistry needed for continuous, restorative sleep.
What's Really Happening – The Science of Sleep Onset vs. Sleep Maintenance

At a glance, how sleep actually works. In reality, it is a highly organized process. Falling asleep is a controlled shutdown of wake systems. Staying asleep is the job of networks that keep that state stable as the brain cycles through different depths of sleep.
Sleep‑onset insomnia describes trouble initiating sleep even when there is time and a chance to sleep. Sleep‑maintenance insomnia describes repeated awakenings, long periods of middle‑of‑the‑night wakefulness, or very early morning awakenings that do not allow a return to sleep. Both fall under insomnia, but they involve different weak spots in the system.
Sleep architecture is the term for how the brain moves through sleep stages in cycles that last about ninety minutes:
-
N1: Very light sleep, easy to wake from; the “dozing” phase.
-
N2: Light to moderate sleep; body temperature drops and heart rate slows.
-
N3 (deep sleep): The deepest, most restorative non‑REM sleep, key for physical recovery and immune health.
-
REM (rapid eye movement): Critical for memory, mood regulation, and emotional processing.
The brain has to both enter this cycle and then keep moving through it smoothly.
Many people assume any sleep problem should respond to the same pill or the same dose of melatonin. Once the underlying biology is clear, it becomes obvious why that rarely works. The chemistry that lets the brain let go at 10 p.m. is not identical to the chemistry that keeps sleep solid at 3 a.m.
As the American Academy of Sleep Medicine puts it, insomnia is “difficulty falling asleep, staying asleep, or waking up too early, with daytime impairment” — not just a matter of short nights.
The Neuroscience of Falling Asleep
To fall asleep, wake‑promoting circuits have to quiet down while sleep‑promoting circuits gain the upper hand. A key player here is GABA, the main calming neurotransmitter in the brain. When GABA activity increases, it dampens firing in arousal centers, so brain activity shifts from sharp and fast to slower and more synchronized.
Melatonin enters as a signal that night has arrived. It does not knock someone out; it tells the internal clock that this is the window when sleep should happen. Adenosine, a natural by‑product of being awake, has been building up all day and now pushes heavily toward sleep. At the same time, cortisol, the main stress hormone, is supposed to drop to its low point so it no longer shouts “stay alert.”
On an electrical level, brain waves shift from beta (focused wakefulness) and high alpha (relaxed wakefulness) into theta, the lighter stage of sleep. When someone is in a state of hyperarousal, cortisol stays high, GABA signaling is outmatched, and the brain remains stuck in fast, alert patterns. The result is that heavy, wired‑and‑tired feeling where the body begs for rest but the brain will not release control.
The Neuroscience of Staying Asleep
Once sleep begins, the job changes from flipping the switch to keeping the system stable. The brain now moves through repeated cycles of N1, N2, N3, and REM. In healthy sleep, more deep N3 sleep appears early in the night, while REM sleep lengthens toward morning. Each transition between stages is a natural “loose seam” where waking is more likely.
To stay asleep, GABA activity needs to remain strong through the night. Melatonin continues to be released from the pineal gland, keeping the night signal steady. Serotonin, which is a building block for melatonin and a regulator of mood and sleep depth, also plays a role in how solid and restorative non‑REM sleep feels.
During the later part of the night, the brain becomes more sensitive to internal and external noise. Blood sugar dips, bladder signals, pain, or rising cortisol can all push someone from light sleep into full wake. Systems such as the endocannabinoid system (including CB1 receptors) and patterns like alpha brain waves help maintain a calm, stable background that supports continuous sleep. When that background is weak, even small triggers can break sleep wide open.
Why You Can't Fall Asleep – Common Causes of Sleep-Onset Insomnia

When falling asleep is the main struggle, the core pattern is usually simple. Either the brain is too activated, or the timing signal for sleep is off, or both. The sleep system wants to shift into a quiet, synchronized mode, but something keeps pressing the gas pedal.
Common drivers of sleep‑onset insomnia include:
-
Mental hyperarousal
Work worries, health fears, and late‑night planning keep the mental overstimulation. Instead of drifting into slower theta waves, the brain stays in alert beta and high alpha rhythms. People describe this as not being able to “shut off” their thoughts, even when they feel exhausted. -
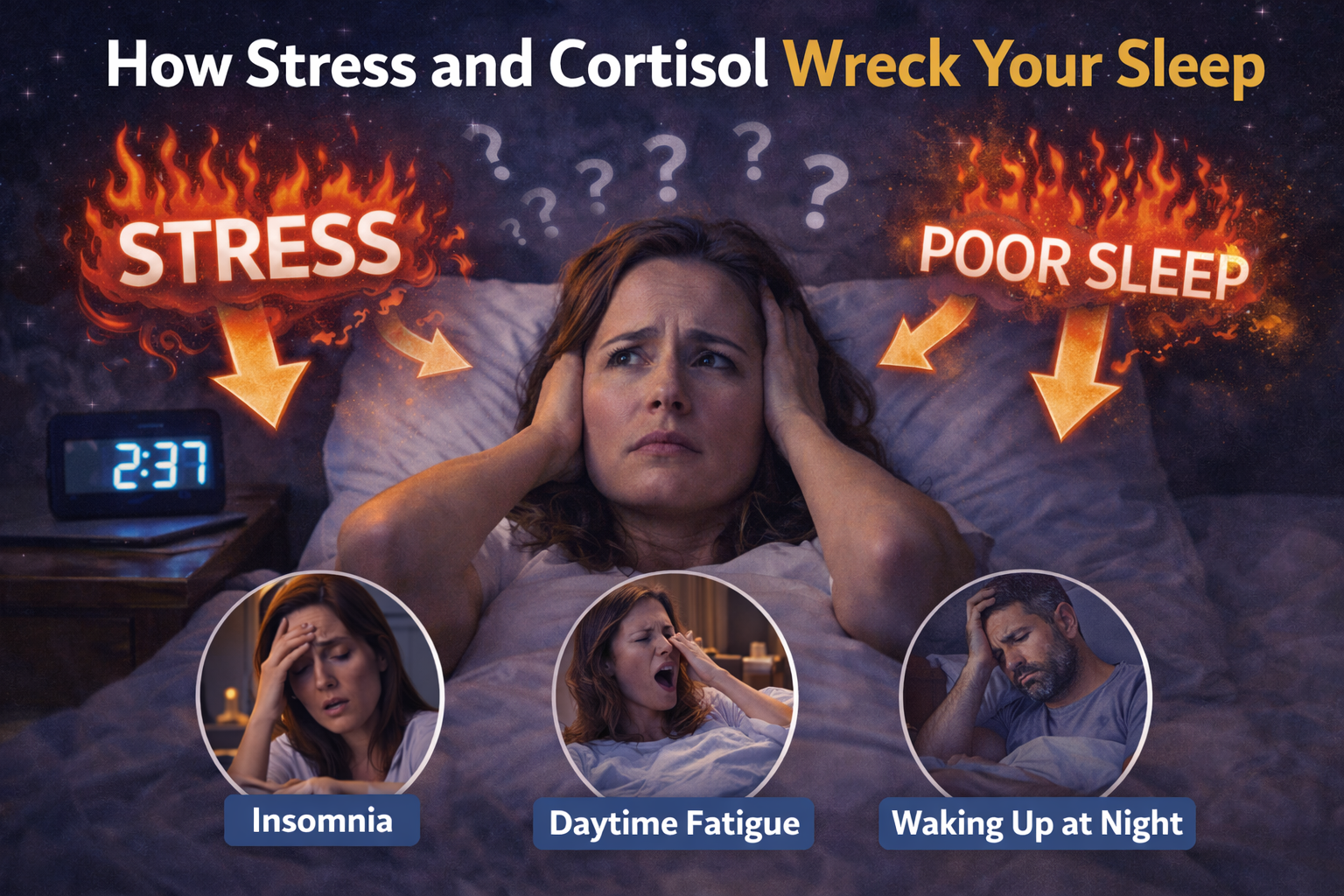
Stress hormones out of sync
Cortisol is meant to be higher in the morning and low at night. When stress is chronic, that curve can flatten or even flip, leaving cortisol elevated in the late evening. That signal tells the body there is a problem to solve, not a time to sleep. It directly counters the calming effect of GABA and blunts the rise of melatonin. -
Circadian rhythm misalignment
Shift work, frequent time zone changes, or a chronic “night owl” schedule push the internal clock later. The brain may not start releasing melatonin until well after midnight, while work or family life still demands an early wake time. In this case, the problem is less about the ability to sleep and more about mis‑timed sleep pressure. -
Evening behaviors that keep the brain “on”
-
Caffeine has a long half‑life and can still block adenosine six to eight hours later.
-
Nicotine is a stimulant, especially for people who do not use it all day.
-
Bright screens in the last one or two hours before bed send a strong daylight signal to the brain and suppress melatonin release.
-
Intense late‑night workouts, emotional conversations, or doing work emails in bed keep the nervous system in a state that is far from sleep.
-
-
Sleep environment and performance anxiety
A hot bedroom, street noise, light leaking through gaps, or an uncomfortable mattress keep the body from settling. When this pairs with anxiety about sleep performance, people start to dread bedtime. Worry about not sleeping becomes its own trigger, feeding the very pattern they fear.
Why You Can't Stay Asleep – Common Causes of Sleep-Maintenance Insomnia
Sleep‑maintenance insomnia looks different. Here, falling asleep is not the main issue. The person may drift off easily, only to wake several times a night or wake once around 2 to 4 a.m. and feel completely alert. The depth and continuity of sleep, not the starting point, are the weak links.
Major contributors to sleep‑maintenance insomnia include:
-
Incomplete nervous system unwinding
Someone may fall asleep because they are exhausted, but their body never reaches a truly deep, parasympathetic state. Sleep stays light and fragile. Minor triggers such as a partner rolling over, a dog moving at the foot of the bed, or a small worry drifting through the mind are enough to push them into full wakefulness. -
Hormonal shifts
During perimenopause and menopause, fluctuating estrogen and progesterone alter thermoregulation and sleep control. Hot flashes and night sweats are obvious wake triggers. Pregnancy and certain points in the menstrual cycle can create similar patterns through changes in body temperature, breathing, and comfort. -
Underlying medical conditions
-
Chronic pain from arthritis or back problems can peak when the body is still.
-
Gastroesophageal reflux may worsen when lying flat, causing burning or coughing.
-
Sleep apnea repeatedly interrupts breathing, forcing the brain to wake just enough to reopen the airway, sometimes hundreds of times.
-
Restless legs syndrome can cause an irresistible need to move, breaking both sleep onset and maintenance.
-
Nocturia from prostate or bladder issues leads to repeated bathroom trips.
-
-
Lifestyle factors such as alcohol and blood sugar swings
Alcohol is a classic example. It may help someone fall asleep faster, but as the body clears it a few hours later, it disrupts REM sleep and pushes the brain into lighter stages. This “rebound” effect often shows up as waking in the second half of the night. Blood sugar swings can do something similar. A very high‑carb dinner or late dessert can lead to a quick spike and then a sharp drop overnight, which the body interprets as a stress signal. -
Age‑related changes
Older adults tend to spend less time in deep N3 sleep and more time in lighter stages. The internal clock may shift earlier, so they get sleepy sooner but also wake earlier. When sleep is already shallow, outside noise, pain, or internal signals have a much easier time breaking through.
The "Three Ps" Framework – Understanding Your Sleep Problem's Origins
Chronic insomnia rarely appears out of nowhere. Sleep specialists often use the “Three Ps” model to map how a short‑term issue turns into a long‑term pattern. This framework looks at predisposing, precipitating, and perpetuating factors, and it can be very helpful when sorting out different types of insomnia, including falling asleep vs staying asleep issues.
-
Predisposing factors
These are the background traits that make someone more likely to develop insomnia. For some people, sleep problems run in families. Others are natural light sleepers or have nervous systems that react strongly to stress. Personality traits such as high concern about performance or a strong tendency to worry also keep the system closer to the insomnia line even in calm times. -
Precipitating factors
These are the triggers that start the problem. They might be a divorce, a new baby, a job loss, a serious illness, a move, or months of demanding deadlines. Travel across time zones or rotating shifts can act as strong circadian shocks. During this period, sleep becomes shorter, more fragmented, or hard to initiate, and the person may feel that their old “good sleeper” identity has disappeared. -
Perpetuating factors
These are the habits and thought patterns that keep insomnia going after the initial stress has faded. People start going to bed earlier and sleeping in later to “catch up,” which weakens their sleep drive. They nap during the day, spend long periods awake in bed, or bring laptops and televisions into the bedroom. Some use alcohol to force sleep, which then disrupts later cycles. Thoughts like “If I do not get eight hours, tomorrow will be a disaster” add performance pressure. Over time, the bed becomes linked with frustration and anxiety rather than rest.
Cognitive behavioral approaches for insomnia focus heavily on these perpetuating factors, because they are the most changeable. Looking at your own Three Ps can show whether your main problem is new and tied to a recent event, or whether it has settled into a more fixed pattern that calls for structured retraining.
Recognizing Your Pattern – Symptoms and Daytime Consequences
Before any strategy can be chosen, it helps to name what is actually happening at night. Sleep‑onset and sleep‑maintenance insomnia can overlap, but one is often more dominant. A simple way to sort this out is to pay close attention to the first thirty minutes in bed and the second half of the night.
Sleep‑onset symptoms often include:
-
Lying awake for more than thirty minutes most nights
-
Feeling physically tired but mentally wired
-
Watching the clock inch forward
-
Noticing a burst of energy right at bedtime
-
A racing mind that brings up work, relationships, and health worries exactly when it is time to relax
The longer someone lies awake, the more anxious they may feel about the time passing.
Sleep‑maintenance symptoms often include:
-
One or more awakenings during the night
-
Waking once and not returning to sleep for an hour or more
-
Waking three or four times, sometimes from dreams, noise, pain, or for no clear reason
-
Regular waking around 2 to 4 a.m. and feeling stuck in a state that is not fully awake but not truly asleep
No matter which type is stronger, daytime effects often look similar. Many people describe mental health, or a sense that simple tasks take more effort. Short mood, and increased anxiety are very common. So are low mood, less motivation to socialize or exercise, and more mistakes at work. Sleep experts care a great deal about these daytime signs, because true insomnia is defined not just by how the night looks, but by how life feels the next day.
If a person asks themselves one question, this one helps: “Is my main struggle the start of the night, or the middle and end?” That answer steers them toward sleep‑onset or sleep‑maintenance strategies, and toward the specific parts of the SLP1 protocol that match their real pattern.
Evidence-Based Strategies for Sleep Onset – How to Get to Sleep Faster

When the main issue is getting to sleep in the first place, the aim is not to knock the brain out. The aim is to create the conditions where the natural sleep switch can flip on its own. That means lowering arousal, lining up the clock, and strengthening the association between bed and sleep.
A central tool here is stimulus control, a core piece of Cognitive Behavioral Therapy for Insomnia (CBT‑I). The idea is simple but powerful:
-
Go to bed only when truly sleepy, not just tired of the day.
-
Use the bed only for sleep and intimacy, not scrolling, shows, or emails.
-
If sleep does not come within about twenty minutes, get up, go to another dim room, and do something quiet until sleepiness returns. Then return to bed.
-
Repeat this pattern consistently, even if it feels odd at first.
Over days and weeks, this retrains the brain to reconnect bed with sleep rather than wakeful frustration.
The American College of Physicians recommends CBT‑I as the first‑line treatment for chronic insomnia in adults, ahead of sleep medications.
The evening environment and routine also matter a lot for sleep onset:
-
A cool bedroom (usually mid‑sixties Fahrenheit) supports the natural drop in core body temperature that helps people drift off.
-
Darkness signals the brain to release melatonin, so it helps to dim lights in the last hour before bed and limit direct screen exposure.
-
Gentle wind‑down activities such as light reading, stretching, or a simple mindfulness practice give the nervous system time to shift gears.
Addressing the body clock directly is often overlooked:
-
Getting bright light outdoors within an hour of waking helps anchor the circadian rhythm.
-
Keeping wake and bedtimes fairly consistent, even on weekends, stops the internal clock from drifting.
-
Avoiding strong light late at night and cutting caffeine by mid‑afternoon removes some of the biggest brakes on melatonin and adenosine signals.
Targeted nutritional support can make these behavioral changes easier to feel. SLP1 Get to Sleep uses ingredients chosen to support the exact chemistry of sleep onset:
-
Apigenin from chamomile helps support GABA receptors and mental calm.
-
Phosphatidylserine can help smooth out elevated evening cortisol.
-
Herbal nervines such as lemon balm and passionflower gently support the calming side of the nervous system.
For people whose main issue is mis‑timed circadian signals, SLP1 Melatonin Nasal Spray uses low doses in a fast‑acting format, helping the brain recognize that it is time to sleep without flooding the system with excessive melatonin.
Across all of these methods, consistency matters far more than intensity. Many people notice changes in how quickly they get to sleep within two to four weeks when they combine behavioral retraining with the right kind of support for their specific biology.
Evidence-Based Strategies for Sleep Maintenance – How to Stay Asleep All Night
When the problem is staying asleep, the target shifts from the moment of sleep onset to the depth and stability of sleep across the night. Here, the focus is on winding the nervous system down more completely, smoothing triggers like blood sugar swings and alcohol rebound, and supporting the brain chemistry that keeps sleep stitched together.
Deep nervous system unwinding starts before lights out. Practices such as yoga nidra, slow progressive muscle relaxation, or gentle restorative yoga in the evening can move the body into a parasympathetic state where heart rate, breathing, and muscle tension all drop. A warm bath followed by a cool bedroom helps the body shed heat, which supports deeper sleep. This level of relaxation makes it less likely that minor internal signals will push the brain into full wakefulness at 2 a.m.
Evening food and drink choices play a quiet but powerful role:
-
A dinner that includes protein, healthy fats, and fiber leads to steadier blood sugar through the night.
-
Very large meals, heavy alcohol, or late sugary snacks can set up spikes and crashes that trigger a stress response a few hours later.
-
Some people find that a small protein‑rich snack a little before bed reduces middle‑of‑the‑night awakenings linked to low blood sugar.
Alcohol needs special mention. It can make sleep come quickly, but it fragments sleep later by disrupting REM and pushing the brain into lighter stages as it wears off. Many people with middle‑of‑the‑night awakenings notice that keeping a three‑hour gap between their last drink and bedtime reduces these wake‑ups. Swapping late drinks for herbal teas such as chamomile can support relaxation without the rebound effect.
Addressing medical and hormonal drivers is also key. Treating sleep apnea, managing reflux with meal timing or bed elevation, and working with a clinician on pain control or hormone therapy can change the structure of the night dramatically. For chronic insomnia, sleep restriction therapy, another CBT‑I tool, can help by briefly tightening the time in bed to match the actual amount of sleep, which builds stronger sleep pressure and gradually leads to deeper, more continuous sleep.
SLP1 Stay Sleep and Natural Magnesium Sleep Powder are built for this phase of the night:
-
Magnesium glycinate supports GABA activity, calms the nervous system, and relaxes muscles without acting like a sedative.
-
The broader SLP1 approach includes ingredients that support serotonin and melatonin pathways, CB1 receptor activity, and alpha brain waves that form a calm backdrop for deep non‑REM sleep.
-
The formulas focus on bioavailable forms and meaningful doses rather than trace amounts, which is important when the goal is to stay asleep through the most fragile stages of the night.
The SLP1 Protocol – A Comprehensive System for Both Challenges
Most sleep system focus on one narrow part of the night. SLP1 was designed differently, as a full protocol that looks at the entire arc of rest from the first yawn to the final wake. It separates the chemistry of sleep onset from that of sleep maintenance and then brings them back together in a coordinated way.
The core system includes:
-
Get to Sleep for rapid night signaling and mental calm
-
Deeper Sleep for helping the nervous system relax into deeper stages
-
Stay Sleep for overnight continuity
-
Melatonin Nasal Spray for a precise timing nudge when the clock is off
-
Natural Magnesium Sleep Powder to support deeper, more relaxed sleep, especially for people who fall asleep easily but wake in the night
Personalizing the protocol starts with noticing your main pattern:
-
If falling asleep is the longest, most stressful part of the night, Get to Sleep and the Melatonin Nasal Spray take center stage.
-
If sleep comes quickly but waking at 1 to 3 a.m. is the rule, Stay Sleep and the Natural Magnesium Sleep Powder become the focus.
-
If both falling asleep and staying asleep are problems, pieces can be layered in a simple sequence that follows the night.
The ingredients across the protocol are chosen to synergistic formulas rather than compete:
-
Apigenin from chamomile supports mental quiet.
-
Magnesium glycinate offers a well‑absorbed form of magnesium that calms the nervous system without stomach upset.
-
Phosphatidylserine supports a healthier cortisol pattern.
-
Lemon balm and passionflower act as gentle nervines that support GABA receptors.
-
Melatonin appears only in the nasal spray and in microdoses meant for clock correction rather than heavy sedation.
Just as important as what is included is what is left out. SLP1 avoids common allergens, artificial colors, and extra fillers, and it uses third‑party testing to check for potency and contaminants. That aligns well with people who research ingredients, care about long‑term health, and want sleep support that respects their biology instead of overriding it.
When to Seek Professional Help – Red Flags and Medical Evaluation
Self‑guided changes and thoughtful supplementation can go a long way, but there are times when professional support becomes important. A simple rule of thumb is that if sleep problems have lasted at least three months, happen at least three nights a week, and make daily life clearly harder, it is time to talk with a clinician.
Some red flags point even more strongly toward medical evaluation:
-
Loud snoring paired with gasping or breathing pauses
-
Severe daytime sleepiness even after enough time in bed
-
Waking with headaches
-
Uncomfortable leg sensations that worsen at rest
-
Chronic pain, frequent heartburn at night, or repeated nighttime trips to the bathroom
-
Strong symptoms of depression or anxiety
-
Growing reliance on alcohol, cannabis, or sedating pills to get any sleep at all
During an evaluation, a healthcare provider will usually ask detailed questions about bedtimes, wake times, naps, work schedules, stressors, and health history. They may request a sleep diary or use questionnaires such as the Insomnia Severity Index. If they suspect a disorder like sleep apnea or periodic limb movements, they may recommend an overnight sleep study.
For chronic insomnia itself, Cognitive Behavioral Therapy for Insomnia (CBT‑I) is considered the leading treatment, with many people seeing large improvements over a few months through either in‑person care or structured digital programs.
Conclusion
Falling asleep and staying asleep often get lumped together under one word, insomnia. In reality, they draw on overlapping but distinct brain systems. Sleep onset depends heavily on calming a wired nervous system and sending a clear night signal. Sleep maintenance depends more on deep, stable sleep architecture, steady internal chemistry, and fewer triggers during light sleep phases.
Naming which part is most disrupted is the first meaningful step. Once someone can say “my main problem is the first half‑hour in bed” or “my main problem is waking and not being able to get back to sleep,” they can stop guessing and start choosing approaches that match the actual biology. That includes behavioral strategies such as stimulus control, circadian rhythm care, and nervous system unwinding, as well as thoughtful attention to medical and hormonal factors.
SLP1 was built for people who want that kind of precision. Its protocol respects the difference between falling asleep vs staying asleep and focuses on restoring natural rhythm with clean, tested, in‑house formulations instead of chasing quick fixes. Paired with consistent habits and a bit of patience, most people see clear shifts within a few weeks. Better sleep is not a fantasy or a one‑night miracle. It is a predictable response when the right levers are matched to the right problem.
FAQs
Can You Have Both Sleep-Onset and Sleep-Maintenance Insomnia at the Same Time?
Yes, many people deal with both patterns at once. They may take a long time to fall asleep, then wake in the middle of the night and have trouble returning to sleep. This is especially common once short‑term insomnia has been present for months and has turned into a more fixed pattern. In that case, it helps to combine methods for calming bedtime hyperarousal with methods that deepen and stabilize sleep. SLP1’s full protocol was designed with this mixed picture in mind, using Get to Sleep for onset and Stay Sleep for continuity.
Is It Normal to Wake Up Once or Twice During the Night?
Brief awakenings between sleep cycles are normal, and most people do not remember them. The brain naturally comes up to a lighter state every ninety minutes or so, checks the environment, and then drifts back down. This does not count as insomnia when it is short and not distressing. The concern begins when awakenings are long, frequent, or cause worry, or when they lead to feeling unrefreshed and impaired the next day.
Does Melatonin Help With Staying Asleep, or Just Falling Asleep?
Melatonin is best understood as a timing signal for the internal clock rather than as a strong sleep drug. It helps the brain know when night starts, so it can be very useful for shifting sleep onset earlier or easing jet lag. It is less effective for keeping someone asleep through the night, because it does not directly deepen sleep the way GABA and related systems do. Very small doses, often around a third of a milligram, are usually enough for this signaling role. SLP1 focuses on microdosed, fast‑acting melatonin in a nasal spray for timing support, while using other ingredients to support the chemistry of sleep maintenance.
Why Do I Wake Up at the Same Time Every Night, for Example 2 a.m. or 3 a.m.?
Waking at a consistent time often lines up with the structure of sleep cycles. Around the second half of the night, the brain moves from deeper non‑REM sleep into lighter stages and REM, where it is easier to wake. If blood sugar dips, cortisol begins to rise toward morning, or alcohol is wearing off, that lighter stage becomes even more fragile. Hormonal changes, pain, or a nervous system that never fully relaxed can all amplify this effect. Supporting deeper sleep, steadier blood sugar, and better nervous system calm through methods such as SLP1 Stay Sleep and solid evening habits often reduces these patterned awakenings.
What's the Difference Between SLP1's Get to Sleep and Stay Sleep Formulations?
Get to Sleep focuses on the first part of the night. It uses apigenin from chamomile, phosphatidylserine, and calming herbs such as lemon balm and passionflower to support GABA activity, ease mental chatter, and smooth excess evening cortisol, all of which help with falling asleep.
Stay Sleep is designed for the middle and later parts of the night. It leans on magnesium glycinate and other ingredients that support GABA and serotonin pathways, CB1 receptor activity, and alpha brain waves that keep sleep deep and stable. They are meant to be different on purpose, so they can be used alone for a specific problem or layered together for full‑night support.

{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.